Case Report: 57 year old female, small frame. At age 28, she was diagnosed with uterine cancer and after a complete hysterectomy, she was treated with radiation. It’s important for this case to know that menopause began following the hysterectomy, much earlier than usual. She was never consistently prescribed hormone therapy… let’s talk about it.
Two bowel obstructions and surgical interventions throughout her treatment led to the formation of significant scar tissue and more surgeries. She self-referred to me for urinary and bowel incontinence. Grateful to have all the time that we need to take a thorough history (a rewarding benefit of our private clinic setting), she tells me that she had “stopped thinking” about any type of sexual activity since she never thought “it would work” anyways.
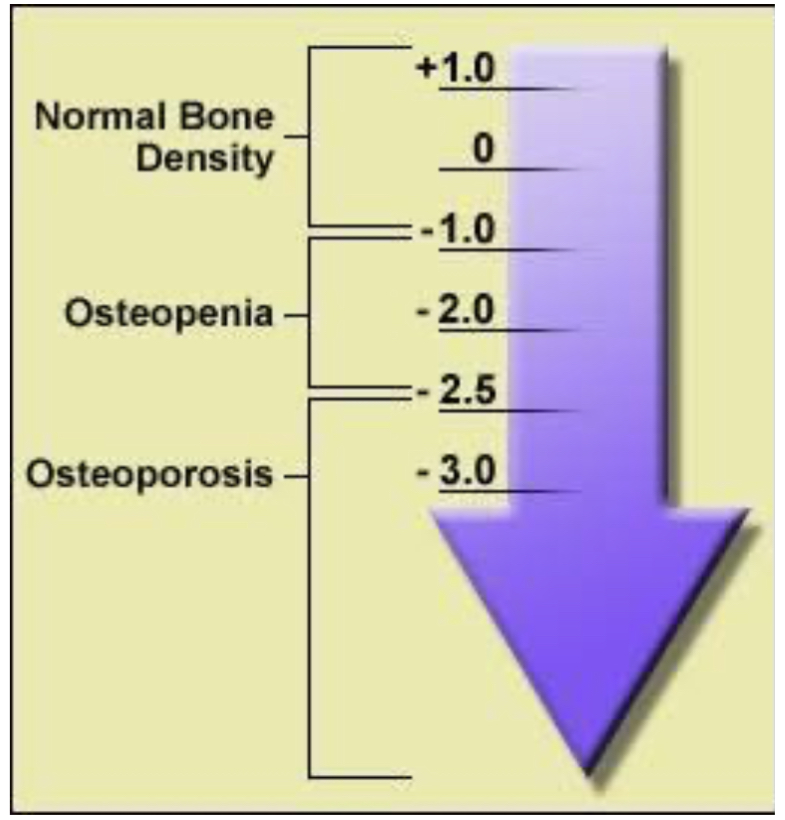
As part of my intake, I asked her about all other health conditions, including bone health. The decline in estrogen during and after menopause accelerates bone loss, and loss of sufficient bone density leads to osteoporosis, a condition that increases fracture risk. She said her PCP told her that her insurance won’t pay for bone density assessment until she’s 65! 😡 Outraged, I called a GYN friend who managed to see her and send her off for her first Dexa scan (a bone mineral density test). Important to note—Dexa index scores of -2.5 or lower indicate osteoporosis (weak bones/high chance of fractures), while scores of -1.0 or higher indicate normal bone density. This patient’s Dexa score? -3‼️
Adequate estrogen levels promote bone formation and maintain bone mineral density; since she went into menopause so early, her chances of having osteoporosis is that much more significant. The lack of action in her 20s/30s that led to this is so troubling. After these results, the doctor and I confirmed the treatment plan (also considering her pelvic-related issues) and got her started with hormone therapy. While hormone therapy isn’t always for everyone, her care team should have thought about assessing her bone health many years ago. That association is very clear—no estrogen ➡️ bone density loss.
The key takeaway here is that interventions could have been done to help her bone health and other subsequent complications. As medical professionals, our responsibility is to our patients—not insurance companies. It is our duty to use the investigative skills we were trained in to make our patients’ outcomes better, focusing on prevention as much as possible! 👏